


R&R #11: GLP-1 inhibitors - The Value of Collectively Targeting Metabolic Aging Diseases
Will the greater takeaway from GLP-1 drugs be that science truly can give us more control over our health as we grow older?

Metabolic syndrome describes broadly a number of comorbid aging-associated diseases such as heart failure, type-2 diabetes (T2D) and its complication, MASH (Metabolic-dysfunction Associated Steatohepatitis, formerly known as non-alcoholic steatohepatitis or NASH), chronic kidney failure, and more. They are linked by ties to the same metabolic pathways associated with insulin receptor signaling and cell growth/repair.

Really the one word today is “metabolic syndrome”, except actually that’s two words…
While thought of as "lifestyle diseases", they are defined by a kind of metabolic tipping point that both age and over-nutrition bring us closer to. As in, for a person with average genetic risk-factors to get T2D as a 35 year old they would need to be morbidly obese and incredibly unhealthy, whereas at 60 they most likely need to be at least somewhat health conscious to fully avoid it. Given that a large % of the population will always not be Jack Lalanne, these diseases can be thought of at a population level as the "early" aspect of aging, and the average age of T2D onset in the US is 49.9 years (as of 2018). Whereas other aging diseases such as severe immunodeficiency leading to pneumonia/sepsis risk, macular degeneration, etc can begin to develop in late middle age but become very common when people reach their 80s, and are more independent of lifestyle choice.

Metabolic Syndrome Risk by Age in a Sample of 1369 Individuals, Cipullo et al 2014
As earlier occurring aging diseases they also have wider prevalence given that people live more years of their life with the diseases, and the population of 55 year olds is larger than that of 85 year olds. That and the comorbid, multi-disease nature of metabolic syndrome results in a situation where the diseases drive a disproportionate amount of our healthcare system's costs and individuals' woes. Some major examples:
-T2D: 536.6M global prevalent cases (2021)
-MASH: Estimated global adult prevalence of 5% (2024)
-Obesity: Around 1B people globally and trending upward (2024)
Thus as the most widespread, visible, co-morbid and expensive aspect of aging, a proactive approach to treating metabolic syndrome would be game changing.
The aging space thus has a long-track record of interest in multifunctional anti-metabolic syndrome drugs. The two most well known small molecule drugs in the longevity space are arguably metformin and rapamycin, both drugs which target signaling in the broader insulin and growth pathways and improve insulin resistance/metabolic syndrome parameters. There are also other, more recently developed and less widely appreciated protective compounds effective broadly against metabolic syndrome linked diseases. SGLT2 inhibitors like Jardiance and Farxiga are simultaneously transforming treatment for diabetes, heart failure and chronic kidney disease. A recent article in longevity.technology interviews Nir Barzilai, a professor at Albert Einstein College of Medicine known for his work on the TAME clinical trial aiming to test the broad anti aging disease effect of metformin. He believes that metformin, SGLT2 inhibitors, and GLP-1 agonists constitute some of the most relevant examples of gerotherapeutics as they treat multiple age-related indications, increase healthspan and reduce overall mortality in humans.
Note the inclusion of GLP-1 agonists in this list. In the period from late 2022-2024 the layman learned that AI is in fact a thing beyond 2001 A Space Odyssey, investors and companies fomented a positive feedback cycle of obsession with the powerful yet still imperfect technology, and strong opinions one way or another arose left and right. To a slightly reduced extent, the pharma world's equivalent of this tech phenomenon has been weight loss drugs falling in the GLP-1 and GLP-1+ class. Relatives at Thanksgiving talk about Ozempic/Wegovy (semaglutide by Novo Nordisk) and Mounjaro/Zepbound (tirzepatide by Eli Lilly) in a way that simply wouldn't happen with other blockbuster drugs like Humira or Keytruda. People no longer think of weight loss drugs as implying glorified caffeine pill snake oil, and various Hollywood celebrities tout their considerable benefits for weight loss.
As Novo Nordisk and Lilly forge ahead, investment is booming in finding ways to increase the potency, ease-of-use, and safety/tolerability of the drug class, with many different companies having something in the pipeline. Beneath the noise, though, the real value of these drugs is in their benefit to metabolic syndrome as a whole rather than just the benefit for obesity. Tirzapatide (Mounjaro for diabetes and Zepbound for obesity) has been shown in a Phase 2 trial to be beneficial in MASH. It also majorly reduced heart failure hospitalizations and deaths by 38% in a Phase 3 trial. The following is a non-exhaustive list of aging disorders that GLP-1 agonists are being tested for:
Type 2 Diabetes Mellitus: Semaglutide and tirzepatide both approved
Obesity: Semaglutide and tirzepatide both approved
MASH: Semaglutide: Pre-NDA, tirzepatide: Phase 2 success
Cardiovascular Risk Reduction in Obesity patients: Phase III success for semaglutide
Early Alzheimer’s Disease/Mild Cognitive Impairment: Semaglutide: Phase III, and good results thus far with liraglutide in smaller trial
Parkinson’s Disease: Some Phase II success with Lixisenatide
Chronic Kidney Disease: Phase III success with semaglutide
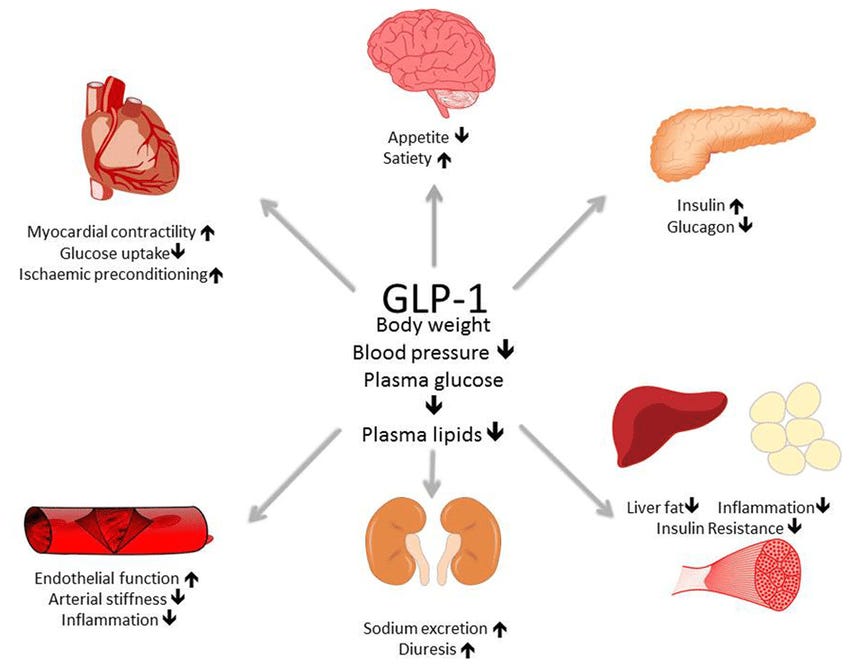
Various Tissue Level Benefits of GLP-1
What differentiates GLP-1 and GLP-1+ agonists versus the other compounds such as rapamycin and metformin listed is that as noted, GLP-1 drugs have reached the world stage faster and more impact-fully than most any other medicine. Having come to the market only over the course of the last half decade, semaglutide earned Novo Nordisk ~$15.4B in the first 9 months 2024, and tirzepatide earned Lilly $11B in the first 9 months of 2024.
But in addition to their commercial and medical value, these drugs also are able to transform opinions due to the media attention they garner and their direct proximity to our day to day lives. These are Reddit front page material, not just for biohackers. In fact, we probably almost all know someone at this point who has taken or is taking either semaglutide or tirzepatide for obesity, and the effect may be more visibly dramatic than those of many other medications. You can't see someone's Crohn's Disease being cured by Humira, but you can see the 50 pounds they lost on Zepbound.
There already is coverage beginning on this topic in mainstream media even as the tertiary indications and beyond remain in the trial stage, for example where The Economist just recently asserted that they may be some of the most important breakthroughs in modern medicine. Recently Elon Musk, who has himself taken GLP-1's for weight loss, stated that he believed that "Nothing would do more to improve the health, lifespan and quality of life for Americans than making GLP-1 drugs super low cost to the public. Nothing else is even close". So, an important question remains: technical hurdles and existing side-effects aside, will people come to appreciate that these medications are not just weight loss drugs, but potentially a swiss army knife for dealing with metabolic and aging diseases?
If people come to appreciate GLP-1s as a broad spectrum anti-metabolic syndrome success, it may have a positive fallout effect on general interest in longevity medicine. With this level of public support and acknowledgement, combined with potentially many 40-70 years olds we know becoming visibly fit and healthy whereas they were previously in the depths of "early" metabolic aging, will it bring upon people the thought "maybe with science, the decline of my health is not inevitable"? And if so, will people conclude that after they get through "early" aging with their health largely intact, that quickly graying and decaying remains their natural destination? Or will they want more? Only time will tell.