


R&R#4: Life Extension is an Existing Trend
Speculative scenarios from science fiction often outline perceptions regarding the word "life-extension". But what is the scenario like from the ground?

The average human lifespan has been on an upward trajectory for over two centuries, a testament to the remarkable advances in science, medicine, and public health. This journey, marked by significant inflection points, has seen humanity conquer numerous health challenges. What, exactly, makes modern rejuvenation medicine unique, and more controversial in some circles?
One interesting way of looking at it is that there are, in essence, 4 ways to die. This is visualized in the matrix below:
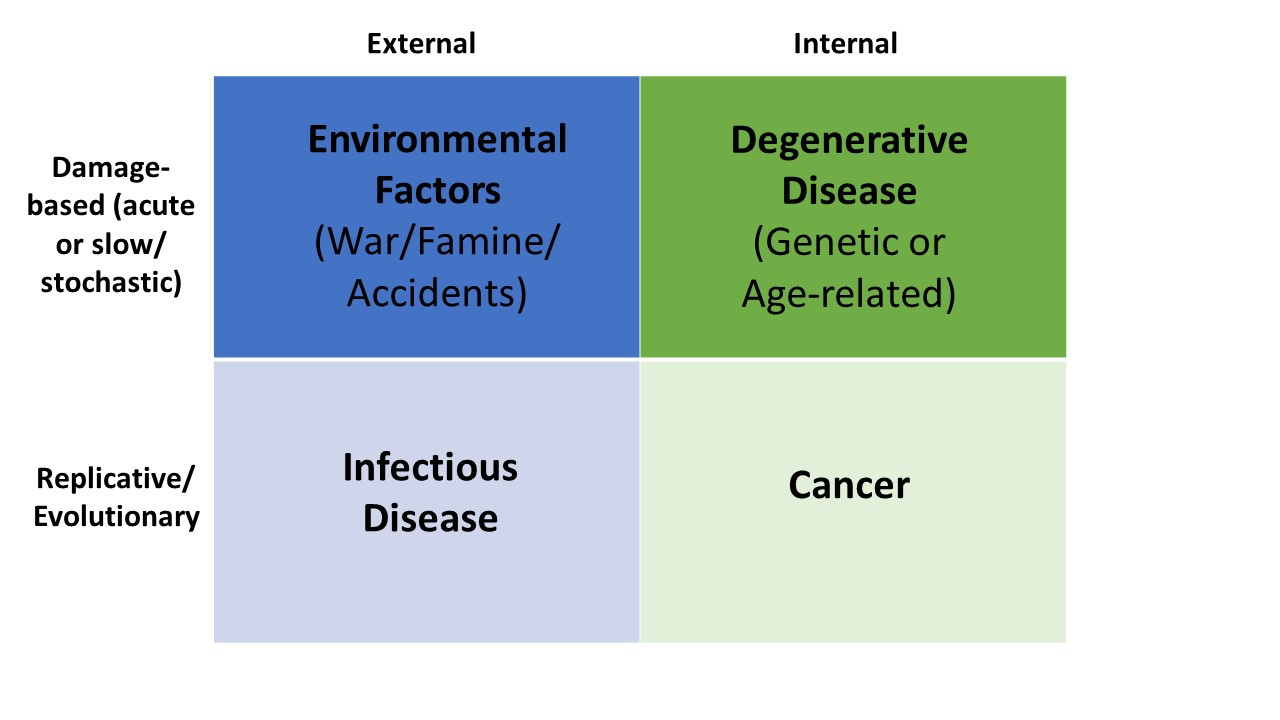
4 Ways to Die, Graphical Overview
These include:
Environmental factors (external origin, damage-based)
Infectious diseases (external origin, replicative/evolutionary)
Cancers (internal origin, replicative/evolutionary)
Degenerative diseases (internal origin, damage-based, includes aging diseases as well as most genetic diseases)
This is more of a way of looking at things than a scientifically testable hypothesis, and there is obviously overlap – immune system degeneration contributes to infections and cancers, environmental radiation can contribute to cancer and potentially aging, etc. Nutritional deficiency also falls somewhere between degeneration and environment, but since its origins are generally due to lack of external resources I would still classify it as an environmental factor. But broadly, two things can be ascertained when one considers this model.
The first is that external origin problems tend to attract more collective attention than internal factors, such as war, climate change, and the pandemic – sensible in the context of an evolutionary history where collective survival was more threatened by these, but now disproportionate in the context of the modern world where most people don’t die of external factors and one of the greatest societal issues is healthcare system failure. Cancer, as a replicative disease, also takes on more attention than degenerative aging given that its onset is sudden and unpredictable, and it is perceived as more unnatural/alien to the body. So, the attention economy very much falls along these lines. The chart below, taken from Our World in Data, reflects this (except for infectious disease, but imagine this was taken in 2020 rather than 2016…)
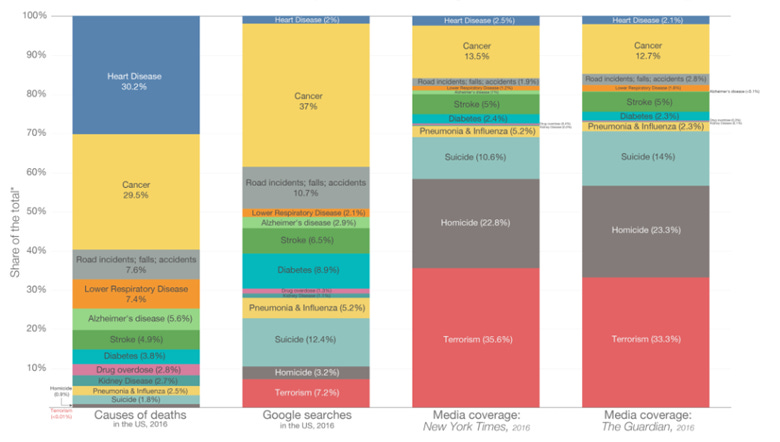
The News Doesn’t Reflect What We Die From, from Our World In Data
The second major thing to realize, though, is that ALL these things contribute to lifespan increase, with each being necessary and none being sufficient. We have had outstanding success reducing external causes of death and recently very good success in cancer, but we’ve had little to no long-term success with degenerative aging disease. Thus, degenerative disease both inspires defeatism in its comparative difficulty, but also carries with it a promise which none of the other 3 revolutions in healthcare has – it is the last firmly planted bolt of a 4-pointed anchor from which death is hanging. Its removal thus carries an air of imminent promise, but in reality, the complexity of the problem means changes will likely be gradual (though hopefully not too gradual).
Let’s consider the history of life extension as measured by mean lifespan increase in the last ~200 years, which is visualized in the chart from “Our World In Data” below. We can see that lifespan in Europe and the Americas stayed relatively flat at ~35 years until around 1870 or so. Then, there was a near linear increase in lifespan since, with lifespan having increased to just over 77 years in 2020*. That’s over double, or around a 43 year increase over a time period of 150 years. That’s around 1 year of life expectancy gained every 3.5 years – not quite Longevity Escape Velocity (LEV, 1 year gained every 1 year), but nonetheless very fast in the grand scheme of things. In some areas it was even faster, like in Asia where the increase started after 1910 and thus was closer to 1 year of life expectancy gained per 2.5 years. Let’s look at a few of the major factors here in terms of the 4 ways to die.
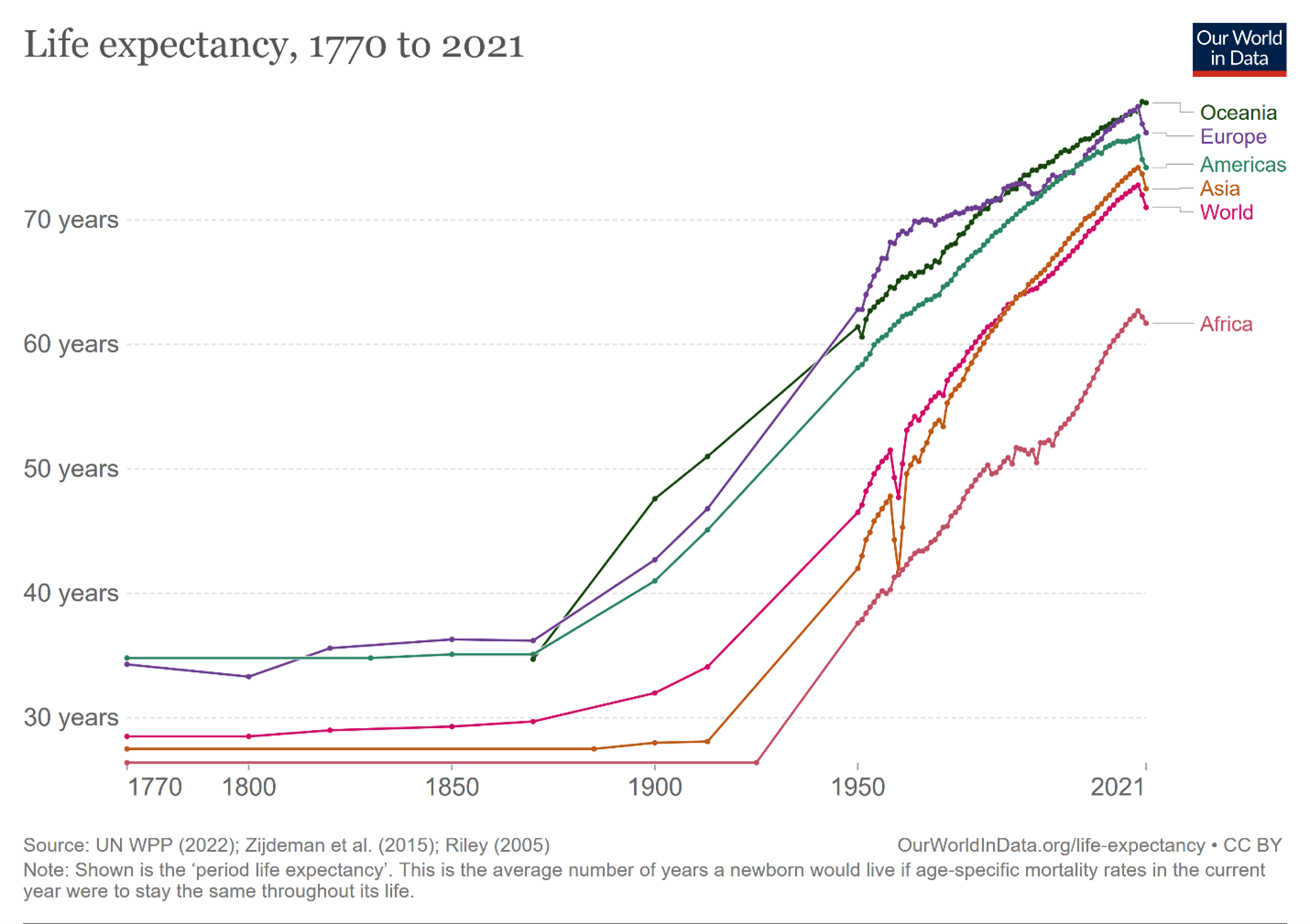
Life Expectancy by Year and Region, Our World in Data
1870 – early 1900’s, External factors (sanitation): At the beginning of the second half of the 1800s, life expectancy remained low in part due to high infant and child mortality rates, with infectious diseases such as smallpox, cholera, and tuberculosis being major culprits. However, the advent of sanitation in the mid-19th century marked a turning point in public health and lifespan. Thus, this represented the first major change which functioned to improve lifespan largely due to changes which reduced exposure to external factors.
First half of the 20th century – Infectious diseases (antibiotics and vaccines): Then, the discovery of antibiotics in the early 20th century was another major milestone and arguably the first which helped defeat diseases rather than prevent them. Sir Alexander Fleming's discovery of penicillin in 1928 revolutionized medicine, providing effective treatment for bacterial infections that were previously often fatal. The emergence of vaccines in public policy, most notably influenza also likely contributed to protection from infectious disease. In 1928 the average life expectancy in North America and Europe was around 50-55 years, and this was seated in the sharpest period of increase on the curve which would be maintained into the beginning of the second half of the century (despite World War II).
1950s – 1970s – External factors (famine and war): Additional important points relating to improved external factors were occurring parallel to these medical advancements.
Most notably, improvements in nutrition, as well as the Green Revolution of the 1960s and 1970s which significantly increased food production, hugely reduced starvation.
Another significant factor in the increase of lifespan which centers around external factors has been the reduction of violence and war. Deaths in state-based conflicts have dropped dramatically since WW2.
Second half of 1900s – Degenerative diseases (hospital care improvement): It was in the latter half of the 20th century, though, that major changes really began occurring in survival for internally originating diseases. Advancements in hospital care, including the development of intensive care units and advancements in surgical techniques, enabled people to live longer by enabling survival under increasing loads of aging damage and disease (though generally didn’t repair the underlying damage).
Post 1950 – Cancer (improved treatments): Additionally, the fight against cancer, a leading cause of death, has also seen significant progress. From the development of chemotherapy and radiation therapy to the more recent advent of immunotherapies and targeted treatments, cancer survival rates have improved dramatically. Numbers for several cancers can be seen in the graph below.
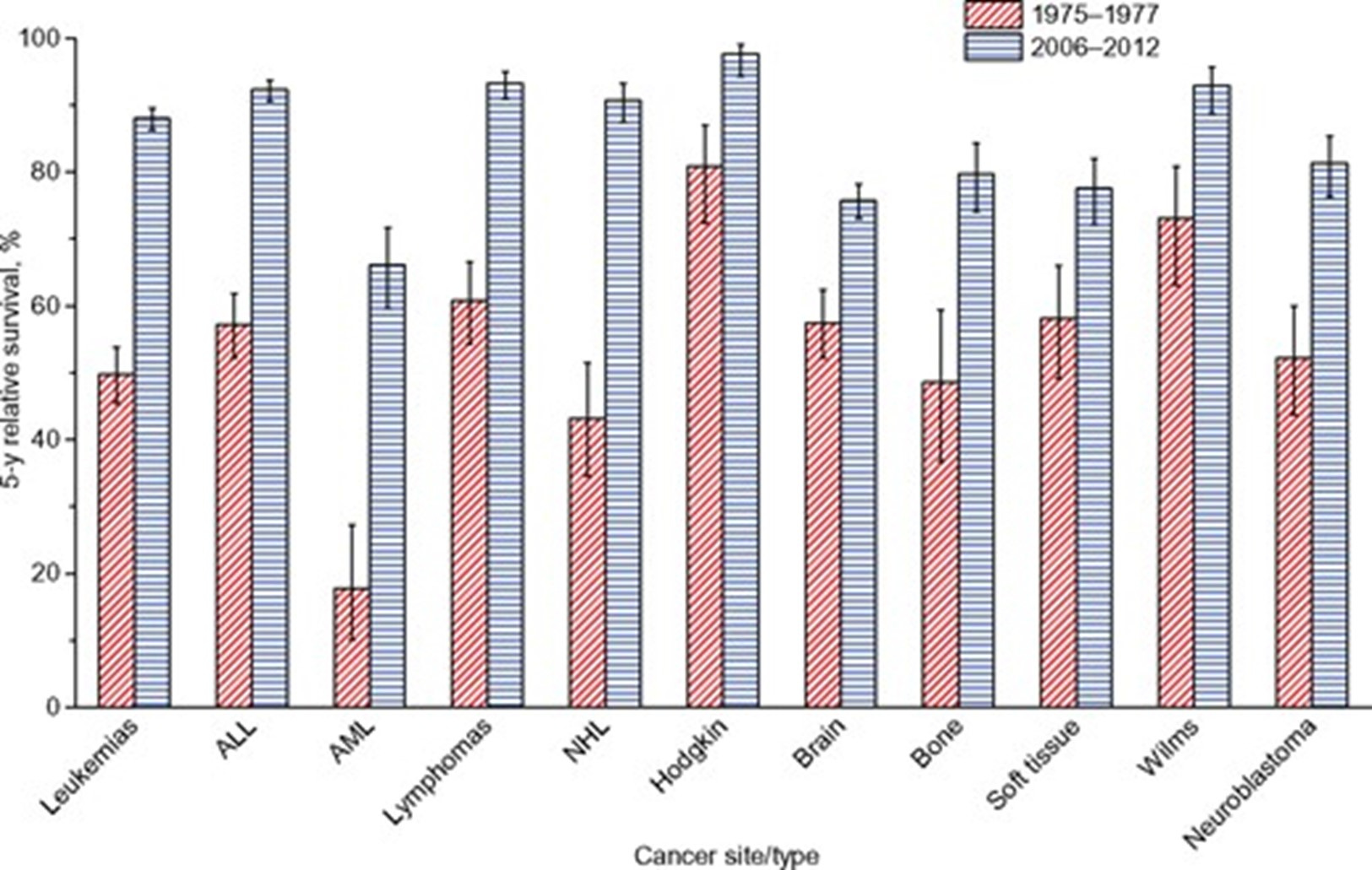
Cancer survival rates have improved over time, Jemal et al 2017
Note that this only extends to 2012 – immunotherapies such as PD1 inhibitors as well as CAR T-cells have made huge inroads in the last several years, and additional targeted treatments as well as blood-test based early detection are likely to further reduce cancer death rates.
2020 – Onwards- degenerative disease (aging therapies): Where do we go from here? We still have room to improve in cancer therapies, and the last few years have shown that pandemics and wars are still a threat. Plus, some areas of the world still need to catch-up and it’s essential that we help facilitate that internationally as best possible. However, both in terms of the most common causes of death that remain in developed countries as well as the least developed area of medicine, it’s clear that age-related degenerative diseases are the next step in the trend. Even in many middle and low income countries, they have become the major killers.
Some aspects of this are universally accepted. For instance, promoting lifestyle factors which are conducive to a long life such as exercise and a healthy diet are a widespread topic of interest. There remains an extra decade of years to grab through this alone if Blue Zone’s like Loma Linda serve as a comparison. Some anti-aging therapeutics like rapamycin could perhaps facilitate this as well. But to push past ~90 years of mean lifespan I expect we will have to utilize direct anti-aging damage therapeutics. Rejuvenation therapies which targets the underlying hallmarks of aging and/or tissue level regeneration, and which actually reduce or eliminate diseases like Alzheimer’s, heart disease, atherosclerosis, chronic kidney disease, autoimmune diseases, and non-alcoholic liver disease.
How fast will these come, and how much could these gain us by the end of the 21st century? If we follow the pre-existing slope broadly, and say 1 year of life expectancy gained every 3.5 years, that would mean we gain just short of 23 years of life expectancy by 2100. This would mean an average lifespan in the US of ~100 years from our current level of ~77 years. On the other hand, many unique factors will factor into how things actually play out. What are factors to consider in regard to whether things will accelerate, decelerate, or remain the same and reach roughly that 103 year level?
There is a higher degree of difficulty in combating aging compared to other causes of death because there are so many associated diseases, each of which will all arise given sufficient time in an individual
Optimistic:
Hallmarks of aging are shared between tissues so therapies may more easily be extended towards other indications
We live in a time where the life sciences research community is large enough that we are able to focus on multiple diseases at once
Pessimistic:
Even one persistent degenerative disease in vital organs or critical vasculature could cap maximum lifespan until it is solved
Brain aging may be a particularly difficult (though not insurmountable) bottleneck due to the relative difficulty of rejuvenation and replacement therapies
The actual timing that robust rejuvenation therapies for aging diseases will arrive on the market remains uncertain
Optimistic:
A thriving aging research and startup community is working on many therapies now, certainly some therapies will come out before 2030
Efforts are being made across hallmarks using multiple strategies
Pessimistic:
Drug development is also a long process, with at least a decade lag in between an initial discovery and a marketed therapy
There will likely be room to improve after the first line of new therapies
There will be a lag between when optimized therapies arrive and when they are widely available. First, due to doctor hesitancy and inertia in the standard-of-care, and then because of challenges in expanding access including supply constraints and the need for international regulatory approvals. It may be longer still until the realization that robust rejuvenation options exist permeates its way across populations.
Optimistic:
One-time or temporary rejuvenation therapies may be more accessibly both economically and logistically than perpetual cocktails of drugs
Powerful therapies may drive urgency towards acceptance among all stakeholders (providers, payers, patients and regulators)
Pessimistic:
The uniqueness of new therapies both in terms of paradigm for clinical use, and in terms of the actual treatment modality (cell therapies, organ replacements, bespoke enzymes, etc) may propel excess caution and slow the rate of adoption
Now, there are many healthy individuals who reach 100 in the US and many who die in their 60s. How will the standard deviation change? In an ideal scenario it will shrink, which would further drive up the mean.
Optimistic:
An increased repertoire of medical options against lifestyle factors driving aging may reduce the current greatest cause of variability
Pessimistic:
Some people may be more interested in living a long-life than others
Black swan events, or unpredictable events with disproportionate effects on long-term outcomes, can occur.
Optimistic:
A body-wide anti-aging strategy, such as a powerful gene therapy, may make a large and sudden shift to maximum lifespan
Less unpredictably, a whole organ rejuvenation or replacement strategy for a critical organ such as the heart or lungs may result in a sudden sharp gain in life expectancy
Pessimistic:
Negative societal changes could quench life sciences R&D and the growth of medicine (the best solution IMO to this is to invest in R&D communities across the globe)
In an optimistic scenario, if the rate of increase doubled to 1 year of life expectancy gained every 1.5 years (1:1 being LEV), it would still appear to someone in 2100 who was looking at a similar graph of life expectancy extending from the 1800s that there was a quantitative rather than a qualitative change in trend. The result would equate to an average lifespan of ~130 years old.
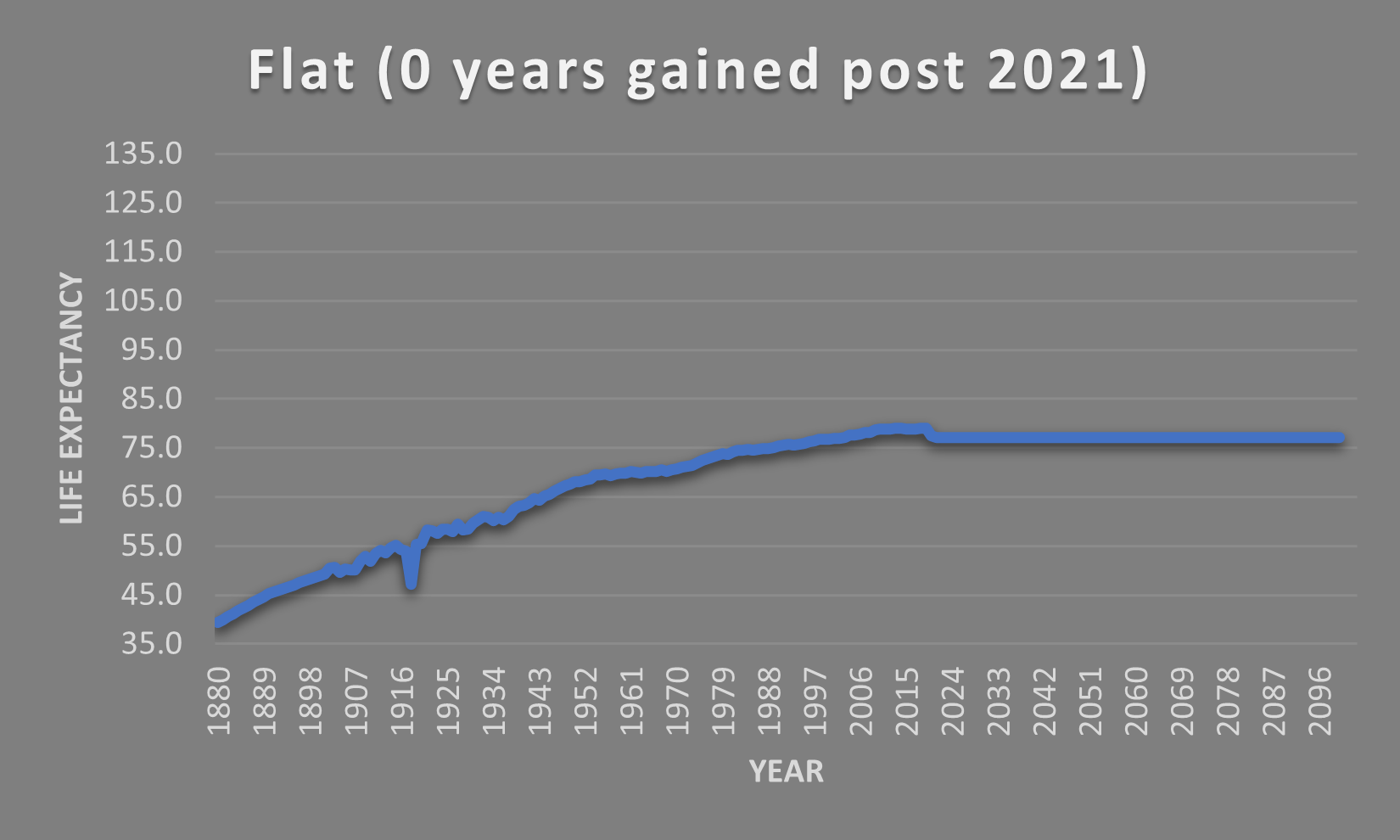

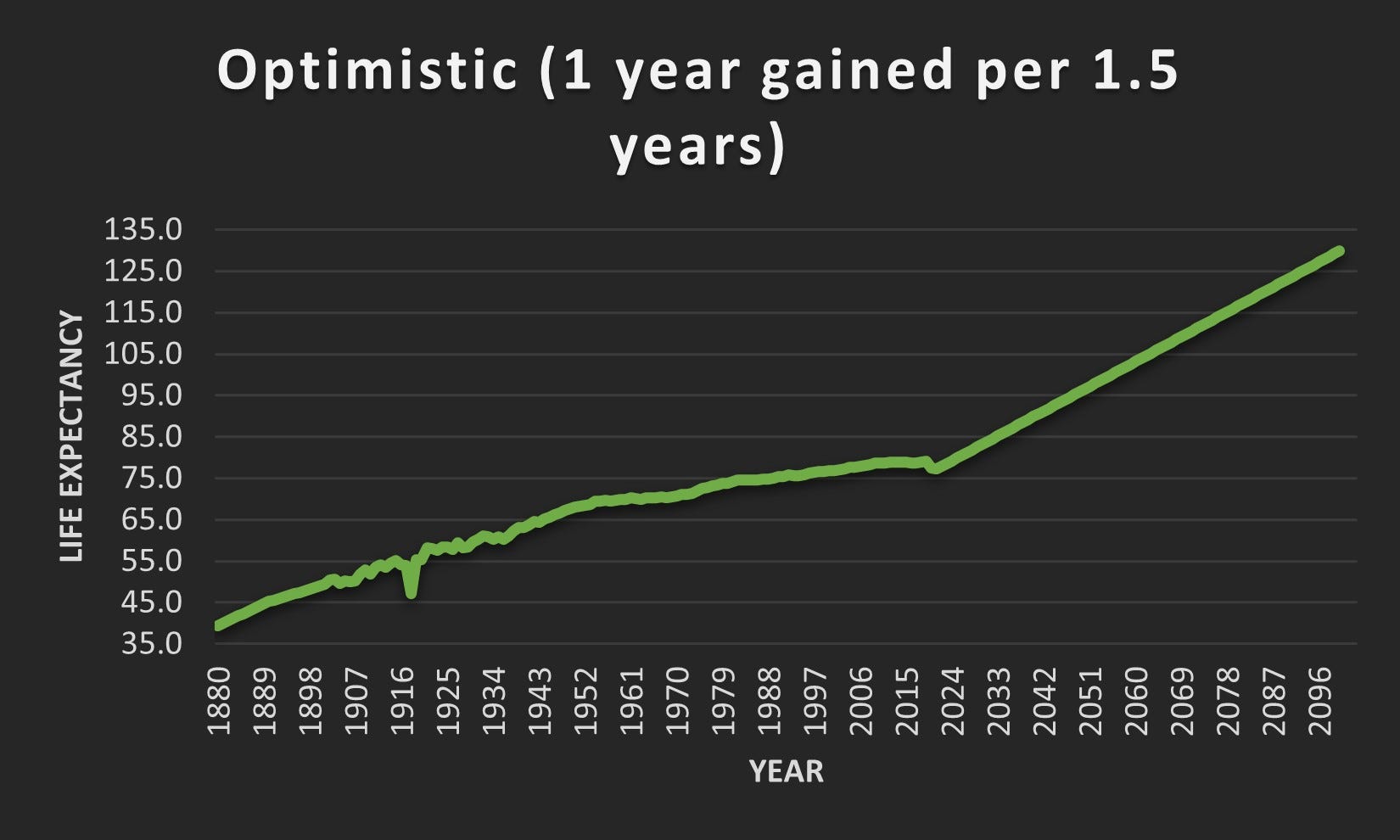
Modelling Lifespan Trends in the US. Data until 2021 taken from Our World in Data. Post 2021 estimates are as listed.
Thus, I believe that the endeavors which the aging research community are focusing on are a continuation of an existing trend of extending human lifespan, as well as the origination of a new trend of targeting degenerative disease with rejuvenation rather than palliative treatment. And they are also likely to bring healthspan more in-line with lifespan, providing a solution to demographic aging and collapsing, overburdened healthcare systems. Arguing over an ideal lifespan is meaningless, and the increase is a natural, historic trend.
That being said, I am still crossing my fingers (and moving my feet) for LEV or better. Regardless, I do believe that college students in 2100 will be as aghast at the imagination of a world filled with hospitals beset with ailing 70 year olds as those of today are at the imagination of streets full of starving 30 year olds and children stricken with polio. Given that I plan to assure that the optimistic timelines are the ones put in place, I also looking forward to telling these students how right they are.